











By Mark S. Gold M.D.
As New Yorkers prepare for one of the hottest Fourth of July weekends in years—with temperatures of 100°F and heat indices exceeding 110°F—public health officials warn of dehydration, heatstroke, and cardiovascular stress. Less appreciated is another danger: Extreme heat may increase the risk that a drug overdose becomes fatal.
For people using opioids, cocaine, methamphetamine, alcohol, or some prescription medications—including diuretics, beta blockers, ACE inhibitors, antipsychotics, and antidepressants—heat can do much more than cause discomfort. It can impair the ability to regulate body temperature, maintain hydration, and survive substance intoxication. Recent evidence shows extreme heat is an underrecognized risk factor for overdose and drug-related emergency visits and deaths, one likely to become increasingly important as climate change brings hotter summers and more frequent and extreme heat waves.
Several years ago, I argued that climate change could become an addiction medicine issue, not simply an environmental one. Rising temperatures, disrupted health care, worsening psychiatric illness, and increased substance use were likely to converge and increase addiction-related illness and death. New research suggests this prediction is already becoming reality.
A national study led by Dr. Julia Dennett and colleagues at Yale University analyzed overdose deaths in nearly every U.S. county between 1999 and 2020 during the summer. Rather than examining air temperature alone, the researchers used the heat index, which combines temperature and humidity to better reflect the body’s physiological heat stress.
Their findings were striking.
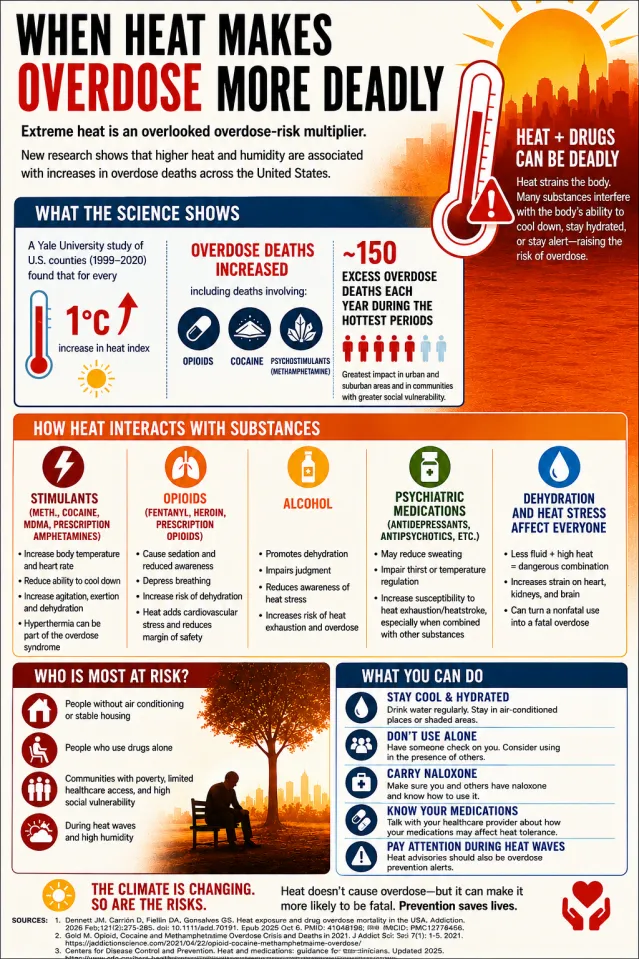
Each 1°C increase in the heat index was associated with a measurable increase in overdose mortality, particularly deaths involving opioids, cocaine, and psychostimulants like methamphetamine. The investigators estimated that approximately 150 excess overdose deaths occur each year during periods of extreme heat. Applied across millions of people during increasingly frequent heat waves, the cumulative effect becomes a meaningful public health burden.
Cocaine-Hyperthermia
As a young cocaine researcher during the cocaine epidemic, I remember patients coming to the emergency room profoundly overheated, agitated, and critically ill from their drug use. Aggressive external cooling—sometimes including ice-water immersion—became standard emergency treatment because lowering body temperature was as important as treating the intoxication itself. The new Yale findings suggest environmental heat may produce a “second hit,” amplifying the toxic effects of opioids and stimulants and contributing to preventable overdose deaths.
Overdose has traditionally been viewed as a consequence of the drug itself—its dose, potency, contaminants, or an individual’s underlying vulnerability. But extreme heat adds another risk factor. By placing additional strain on the cardiovascular, respiratory, and thermoregulatory systems, it reduces the body’s physiological reserve.
Under normal conditions, excess heat is dissipated through sweating and enhanced blood flow to the skin. High humidity, dehydration, many medications, and psychoactive drugs may impair these protective systems. As body temperature rises, the heart works harder, oxygen requirements increase, and dehydration further compromises circulation. A person who might survive drug intoxication under ordinary conditions may no longer be able to compensate during extreme heat.
The interaction differs by drug class. Stimulants—including cocaine, methamphetamine, prescription amphetamines, and MDMA—increase metabolic heat production, elevate heart rate and blood pressure, and impede the body’s ability to cool itself. Individuals may also increase their physical activity, but with reduced awareness of the effects of overheating. Hyperthermia can become part of the overdose syndrome itself, a phenomenon that emergency physicians have recognized for decades.
Opioids pose a different but equally dangerous threat. Respiratory depression remains the leading cause of fatal overdose, but heat magnifies the risk. Dehydration and cardiac stress reduce the body’s reserve, while fentanyl-induced respiratory depression limits oxygen delivery, just as heat increases metabolic demands. Together, these physiological stresses can turn a potentially survivable overdose into a fatal one.
Alcohol and some commonly-prescribed medications further raise vulnerability. Alcohol promotes dehydration and diminishes judgment, making it less likely someone will recognize heat illness or seek help. Certain antidepressants, antipsychotics, and medications with anticholinergic effects interfere with sweating, thirst, or temperature regulation. Combined with recreational drugs, they can substantially increase the risk of heat exhaustion, heatstroke, and overdose during periods of extreme heat.

Emerging Consensus
The Yale study is not an isolated finding. Researchers from California found hotter days were associated with increases in emergency department visits involving opioids, cocaine, and amphetamines. A Canadian study reported higher cocaine overdose mortality during periods of elevated ambient temperature. More recently, a systematic review concluded extreme heat consistently increases emergency health care utilization related to substance use disorders. Different drugs interact with heat through different biological pathways, but the overall conclusion has become increasingly consistent: heat magnifies overdose risks.
The Yale investigators also found the largest increases in overdose mortality occurred in people experiencing homelessness, unstable housing, poverty, limited access to air conditioning, or reduced access to health care. Many use drugs alone, making timely rescue less likely. Others avoid cooling centers because of stigma, untreated mental illness, or fear. In these settings, biological vulnerability and social vulnerability reinforce one another.

Public health agencies routinely issue heat advisories warning older adults, children, and individuals with chronic medical illnesses to stay cool and hydrated. I think that people who use drugs should be considered another high-risk group.
Simple, evidence-informed interventions could save lives during periods of extreme heat. Expanding naloxone availability, establishing hydration and cooling stations, increasing outreach to people experiencing homelessness, reviewing medications that impair thermoregulation (particularly psychotropic drugs), improving access to cooling centers, and encouraging people to avoid drug use during heat waves while connecting them with treatment are practical, relatively inexpensive measures. As extreme heat becomes more common, including these strategies in overdose prevention efforts should become standard public health practice, with costs that are small compared with the human and economic burden of preventable overdose deaths.
Prevention
Overdose prevention has traditionally focused on the drug, the dose, the route of administration (oral, smoked, injected), and the individual. Emerging evidence now suggests a fifth factor deserves equal attention: the heat index and the environment.
Of course, extreme heat does not replace fentanyl, cocaine, methamphetamine, or alcohol as causes of overdoses. But it appears to magnify their lethality by reducing the body’s capacity to withstand them.
References
Dennett JM, Carrión D, Fiellin DA, Gonsalves GS. Heat exposure and drug overdose mortality in the USA. Addiction. 2026 Feb;121(2):275-285. doi: 10.1111/add.70191. Epub 2025 Oct 6. PMID: 41048198; PMCID: PMC12776456.
Gold M. Opioid, Cocaine and Methamphetamine Overdose Crisis and Deaths in 2021. J Addict Sci 7(1): 1-5. 2021. https://jaddictionscience.com/2021/04/22/opioid-cocaine-methamphetamine…
Centers for Disease Control and Prevention. Heat and medications: guidance for clinicians. Updated 2025- https://www.cdc.gov/heat-health/hcp/clinical-guidance/heat-and-medicati…
Benmarhnia T. Commentary on Dennett et al.: When heat and the opioid epidemic collide – implications for climate-resilient public health strategies. Addiction. 2026 Feb;121(2):286-287. doi: 10.1111/add.70302. Epub 2025 Dec 19. PMID: 41416685; PMCID: PMC12779581.
Henderson SB, McLean KE, Ding Y, Yao J, Turna NS, McVea D, Kosatsky T. Hot weather and death related to acute cocaine, opioid and amphetamine toxicity in British Columbia, Canada: a time-stratified case-crossover study. CMAJ Open. 2023 Jun 27;11(3):E569-E578. doi: 10.9778/cmajo.20210291. PMID: 37369523; PMCID: PMC10310343.
Chang HH, Zhang H, Latimore AD, Murray BP, D’Souza RR, Scovronick N, Gribble MO, Ebelt ST. Associations between short-term ambient temperature exposure and emergency department visits for amphetamine, cocaine, and opioid use in California from 2005 to 2019. Environ Int. 2023 Nov;181:108233. doi: 10.1016/j.envint.2023.108233. Epub 2023 Sep 27. PMID: 37897873; PMCID: PMC10712015.
Jhang H, Kim S, Kim K, Choi S, Choe SA. Extreme ambient temperature and emergency healthcare service utilization due to substance use disorders: a systematic review and meta-analysis. Sci Rep. 2025 Apr 19;15(1):13582. doi: 10.1038/s41598-025-98247-x. PMID: 40253512; PMCID: PMC12009368.
Mark S. Gold, M.D., is a pioneering researcher, professor, and chairman of psychiatry at Yale, the University of Florida, and Washington University in St Louis.
Originally published @ Psychology Today