












By Mark S. Gold M.D.
Is preaddiction real? If so, what is it?
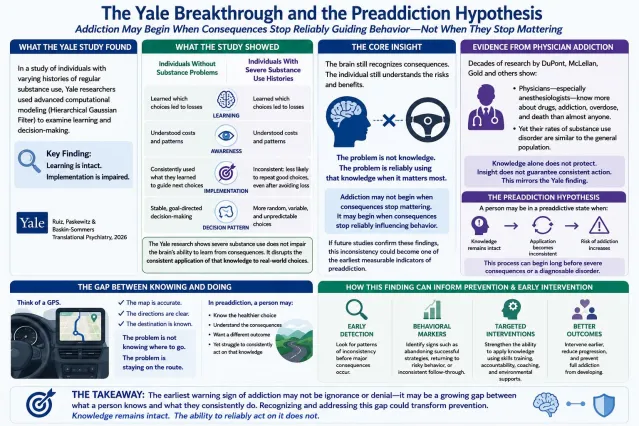
Preaddiction proposes that some addiction-related changes emerge before full substance use disorder develops—and before consequences become severe. Like prediabetes or prehypertension, it suggests a potentially modifiable risk state where earlier intervention may prevent progression to addiction.
Historically, addiction has often been viewed as a progression from experimentation to misuse and finally dependence. Implicit in many models is the idea that severe addiction occurs because people, overwhelmed by reward, deny or become oblivious to consequences.
A recent study from Yale University suggests something much more complex. Using computational models of decision-making, Sonia Ruiz and colleagues found that people with more extensive substance use histories were still capable of learning and recognizing which actions would lead to better outcomes. However, they were less consistent, almost random, in applying what they already knew.
Knowledge remained intact—but its influence on drug use and behavior became less reliable.
Even after making successful choices, they were less likely to repeat advantageous behavior. Participants increasingly shifted toward immediate results, habits, and context-driven responding. Decisions also became more variable and unpredictable.
This distinction matters. These data show addiction may not primarily reflect failure to understand consequences. Instead, addiction may involve impaired translation of knowledge into action. It is also a failure to change current behavior based on already acquired or newly acquired learning.
Patients often say:
“I know this is hurting me.”
“I am destroying my family “
“I know I should stop.”
“I know what I need to do.”
Yet changing their behavior does not follow these insights.
Repeated substance exposure may weaken brain systems involved in integrating prior experience, evaluating delayed outcomes, maintaining goals, and converting intention into action. The result is not a lack of knowledge, but reduced dependability in using that knowledge.
Knowledge Alone Is Not Protective

Evidence for this idea is everywhere, especially in clinical research studies. Physicians—including anesthesiologists and surgeons—command exceptional knowledge about drugs, overdose, and addiction. Yet research for decades has shown that professional knowledge alone doesn’t help doctors reduce their addiction risk. In fact, anesthesiologists have more addiction, overdoses, and drug problems than other physicians.
Understanding the facts about drugs and consistently acting on that understanding are different processes.
The Yale findings offer a possible explanation: The problem may not be whether a person recognizes consequences, but whether learning guides real-world decisions.
Why This Matters for Preaddiction
This is where preaddiction becomes clinically interesting. The earliest change for addicted physicians may not be escalating drug use, but an increasing inconsistency in applying what they know and have learned to future drug use choices. People in a preaddictive state may still function well enough, maintain relationships, work, and want to change.
A person during the transition from preaddiction to addiction may:
- Know healthier choices work—but stop making them
- Experience successful periods of non-use, but these are increasingly harder to sustain
- Have intentions increasingly less predictive of actions
- Change in that consequences become less influential over behavior
My Model
Substance exposure → reduced reliability of using lived experiences and prior learning → unstable decision-making → repeated self-defeating choices → escalating use → addiction.
This hypothetical model requires more study. But if supported, measuring the gap between knowledge and behavior could someday resemble measuring glucose in prediabetes—not diagnostic on its own, but potentially useful for identifying elevated risks.
What to Do
Potential warning signs of preaddiction before addiction becomes entrenched might include:
- Repeatedly abandoning strategies that previously worked well
- Increasing difficulty sustaining healthy choices
- Frequent reversals after positive changes
- An increasing mismatch between goals and actions
Addiction as a Disorder of Risk/Benefit Decision-Making
Modern neuroscience increasingly views addiction as altering brain decision-making mechanisms, not simply excessive pleasure seeking. The brain constantly updates expectations based on experience and adjusts behavior accordingly. The Yale study suggests that with alcoholism and other addictions, this updating process becomes less reliable.
Rather than viewing addiction primarily as a failure of willpower or excessive pleasure-seeking, new models describe addiction as a disorder in how experiences are translated into future decisions.
Computational psychiatry attempts to explain behavior by modeling how the brain updates beliefs, predicts outcomes, and selects actions under uncertainty. Uncoupling knowing and doing starts in preaddiction. Preaddiction learning may occur, but it begins to lose its capacity to update behavior based on knowledge. Also, decoupling lived experience, learnings, and insights is a hallmark of addiction. This mechanistic hypothesis is not metaphorical.
Addiction research increasingly supports the idea of core, altered decision-making processes in which the user experiences losses, learns from them, and understands risks. But paradoxically, learned consequences exert increasingly less influence over future choices.
The brain builds an internal model of the world, estimates future consequences, and chooses actions expected to produce the best outcomes. Repeated substance use shifts behavior away from control and toward model-free responding, where risk/benefit decisions are primarily determined by immediate reward, environmental cues, and previously reinforced routines, rather than explicit knowledge about future consequences. The Yale findings show, from a computational perspective, that prior experience may carry reduced “decision weight.”
With repeated drug exposure, expectations become increasingly centered around obtaining relief, reducing discomfort, or restoring familiar internal states. Addiction-related drug use is highly desired even when consciously recognized as harmful. Preaddiction represents an intermediate state in which learning remains largely intact, but behavioral implementation becomes increasingly unreliable.
Healthy decision-making depends on mentally simulating desired outcomes and allowing those future states to influence present behavior. Substance use disorders appear to be associated with progressively increased discounting of future consequences. The person still knows: “If I keep using, this will likely damage my health.” But that future prediction exerts less influence at the moment of choice.
This new perspective complements instead of replacing existing addiction models involving craving, reward, withdrawal, habit formation, dopamine signaling, and neuroadaptation.

Ramifications for Treatment
If future research supports this model, we should look for the earliest measurable signals of addiction risk—not just craving, intensity, or frequency of use, but an increasing inconsistency between what individuals know, what they intend, and what they actually do.
Treatment may need to focus less on increasing awareness and more on strengthening the use of existing knowledge.
Strategies may include contingency management therapy, recovery coaching, structured accountability, and self-help. Mutual-help groups and recovery communities may function partly as external scaffolding—helping individuals maintain decisions until healthier patterns become more stable. Also, treatment should provide repeated opportunities to practice healthier decisions. Each successful interruption of automatic substance use provides new evidence that using learning to change is possible. Repeated enough times, healthier responses may become easier and more automatic.
So, addiction may not begin when consequences disappear from awareness. It may begin earlier—when consequences remain visible but progressively lose their ability to shape future behavior.
If so, identifying widening gaps between knowledge, experience, and action may become one of the earliest biomarkers and opportunities for prevention and intervention before addiction becomes entrenched.
eferences
Ruiz SG, Paskewitz S, Baskin-Sommers A. The relationship between regular substance use and cost comparisons in stable and volatile learning contexts. Transl Psychiatry. 2026 Jan 30;16(1):103. doi: 10.1038/s41398-026-03830-z. PMID: 41617681; PMCID: PMC12923518.
McLellan AT, Koob GF, Volkow ND. Preaddiction-A Missing Concept for Treating Substance Use Disorders. JAMA Psychiatry. 2022 Aug 1;79(8):749-751. doi: 10.1001/jamapsychiatry.2022.1652. PMID: 35793096.
Ernst M, Grant SJ, London ED, Contoreggi CS, Kimes AS, Spurgeon L. Decision making in adolescents with behavior disorders and adults with substance abuse. Am J Psychiatry. 2003 Jan;160(1):33-40. doi: 10.1176/appi.ajp.160.1.33. PMID: 12505799.
Mark S. Gold, M.D., is a pioneering researcher, professor, and chairman of psychiatry at Yale, the University of Florida, and Washington University in St Louis.
Originally published @ Psychology Today